Aside from the devastating impact that the Coronavirus pandemic continues to have on lives and livelihoods, it’s also had a significant impact on our vocabulary. New terms like COVID-19, self-isolate and social distancing have been added to the dictionary [1], others have taken on new meaning (lockdown, shielding, zoom..), and yet more have seen a surge in use – virus, pandemic, mask, keyworker, carer, hero…
As our lives have changed, so has our language, and we’ve pretty much accepted and adopted this new vocabulary without question. But I have a question. What influence has the language of this pandemic had on our response?
There is one word that has been used ubiquitously over the last few months, and that’s ‘vulnerable’. I want to use this blog post to explore the use of the term vulnerable – particularly during the pandemic – and why I believe its proliferation has done more harm than good.
Vulnerability and ‘the vulnerable’
First, it’s important to emphasise that my frustration and concern here does not relate to people acknowledging or talking about their vulnerability. We are all human. We are all vulnerable. Being open and honest about our vulnerabilities allows us to connect, empathise, share ideas, build friendships, fall in love. To let people in to see who we really are, not what we’re pretending to be.
My frustration and concerns relate to the use of the term vulnerable as a label, and the consequences of this labelling.
The vulnerable label tends to be used interchangeably with other objectifying labels like ‘the elderly’, ‘the disabled’, ‘the homeless’. It’s stuck on individuals (he was very vulnerable, she’s highly vulnerable), applied to groups (vulnerable people, vulnerable children, vulnerable adults) and combined with other labels (vulnerable service user, vulnerable customer, vulnerable case). Often there’s no context – no indication of what it is that the individual or group of people are vulnerable to. And increasingly it’s not obvious that we’re referring to people at all.
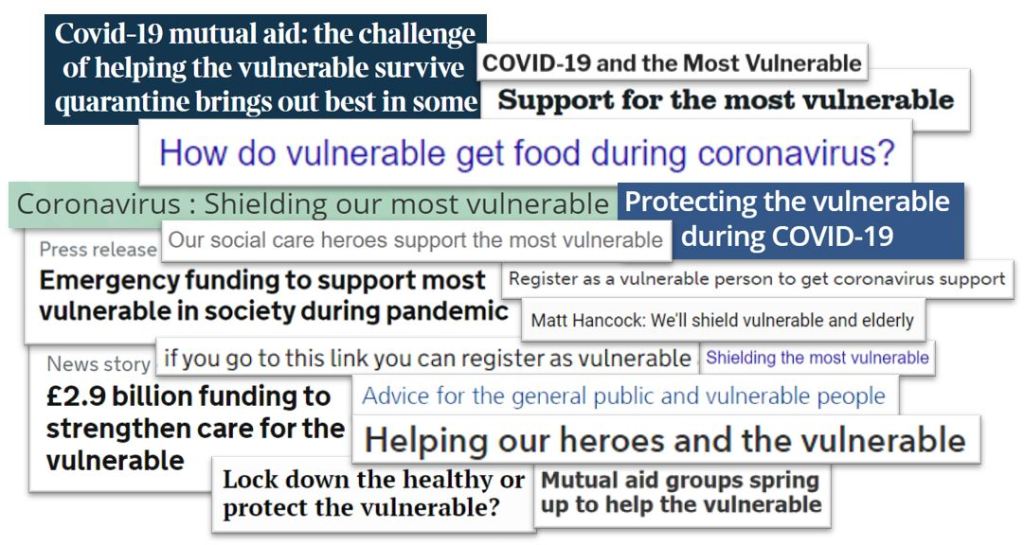
How many times of late have we heard or read phrases like ‘the vulnerable’, ‘the most vulnerable’, ‘our most vulnerable’ or even just ‘vulnerable’ in news reports, articles, guidance, and briefings? The government has issued numerous press releases about new measures to “protect the vulnerable”. Matt Hancock talks repeatedly of protecting “our most vulnerable” and news headlines praise health and social care heroes for “helping the vulnerable”. The humanising noun – person, citizen, resident – is often absent. The adjective has become the noun, with determiners added to group (‘the vulnerable’), rank (‘most vulnerable’) and possess (‘our most vulnerable’).
In the context of COVID-19, the term vulnerable has been adopted to refer to people who are at significantly greater clinical risk from the virus: people who are “clinically vulnerable” or “extremely clinically vulnerable”. But as more is known about the virus, it’s clear that vulnerability from COVID-19 extends far beyond this definition.
The Public Health England report on disparities in the risk and outcomes from COVID-19 identified that you’re at greater risk of serious illness from, or dying with, COVID-19 if you’re older, or male, or have a higher Body Mass Index (BMI), or you live in a more deprived area – or in a care home, or you work in a range of “caring occupations” – including social care, or you’re from a Black, Asian or minority ethnic background, or you’re born outside of the UK or Ireland [2] [3].
The Local Government Association (LGA) briefing for councils on ‘Protecting vulnerable people during the COVID-19 outbreak’ [4] identifies over 40 different groups of people who are vulnerable – or potentially vulnerable – either to the health impacts of the virus or to the consequences of measures to prevent its spread. These groups include: people required to self-isolate who don’t have support from family or friends; people accessing community mental health services; people accessing drug and alcohol services; people who are homeless or who live in overcrowded, temporary, emergency or supported accommodation; unpaid carers; people experiencing or at risk of domestic abuse; people living in more rural settings; people who may experience financial hardship and/or food poverty, and people who are lonely as a result of self-isolation and social distancing.
So, when we (the government, local authorities, the media, charities, banks, supermarkets, the public) blanketly refer to “vulnerable people” – either in relation to, or beyond, the pandemic, do we actually know who we mean? Despite the extent of the impact of this virus on all our lives, the implication is an anonymous ‘them’ – not us. Weak, helpless, hopeless ‘others’. And that’s where it all starts to unravel.
Them, not us
The vulnerable label is not something many people either do – or want to – associate themselves with. As a result, how many of us didn’t sign up for support because to do so meant registering as vulnerable with the government? How many of us didn’t ask for help because we didn’t want to admit our vulnerability?
How many of us faced increased anxiety when we realised the government or our council or our doctor identified us as extremely vulnerable? (Healthwatch Sheffield heard from a person who’d received “daily texts from their GP, reminding them that they are vulnerable and at increased risk of dying if they catch the virus” [5].)
How many of us resented and blamed ‘the vulnerable’ for lockdown? A quick Twitter search reveals tweets like “quarantine the vulnerable – let the rest of us live our lives”, “vulnerable people can just stay inside! Why should the rest of us wear masks??!!”, “protect the elderly & the vulnerable and let everyone else live their life”, and “vulnerable people need to stay at home and keep safe. Let the rest of us live”.
How many of us ignored the messages around hand hygiene and social distancing because we believed we weren’t at risk? We weren’t vulnerable? And as a result, how many of us unknowingly spread the virus?
Blaming people, not situations or circumstances
By labelling people as vulnerable, we’re focusing on individuals or groups as the problem rather than recognising, and addressing, what it is that makes people vulnerable. In labelling and grouping people like this, we’re not just failing to see people as unique individuals – human beings with human rights – we’re also failing to acknowledge or attempt to change the situations or circumstances that create vulnerability.
In terms of COVID-19, the vulnerable label has been used to suggest an inevitability to deaths. Early on we were assured that ‘most’ people would be fine – it was only ‘the elderly’ and ‘those’ with underlying health conditions who were at significant risk. Reports of the first deaths were accompanied by a hasty reference to the deceased person’s age and underlying health condition. There was a distinct ‘they would have died soon anyway’ rhetoric.
In a daily press briefing in early June, Matt Hancock said “From the earliest days of this crisis, we recognise that people in social care were uniquely vulnerable” [6], while England’s chief medical officer Chris Whitty asserted that it was hard to prevent deaths in care homes “because this is a very vulnerable group” [7]. But far from leading to greater measures to reduce risk, it’s becoming increasingly clear that ‘the vulnerable’ were sacrificed. From the initial strategy of ‘herd immunity’ to pressure from doctors for people to sign ‘Do not attempt resuscitation’ notices, the measures introduced in the Coronavirus Act to enable local authorities to ‘ease’ Care Act duties, and the policy to discharge people rapidly from hospital into care homes regardless of COVID status, early legislation, guidance and decision-making effectively wrote off a huge section of the population. Vulnerable = expendable.
Ranking vulnerability
During the pandemic, the focus has been on ‘the most vulnerable’ – an anonymous group rarely defined but implied to be the people on the ‘Shielded patients list’ [8]. This list is collated by NHS Digital and provided to GPs, hospitals and – via the Cabinet Office’s ‘Extremely Vulnerable Persons service’ to local authorities. If you’re on the list, you’re entitled to ‘get coronavirus support as a clinically extremely vulnerable person’ [9]. If you’re not on the list – you’re either not vulnerable enough or you’re the wrong kind of vulnerable.
The LGA paper referenced earlier mentions “the focus of the [local support] hubs will be to arrange help and support for the most vulnerable people in the event of any issues with the centralised arrangements put in place for this group. They are not intended as a general ‘one stop shop’ for all enquiries related to COVID-19 or to support the much wider group of people who have other vulnerabilities or may be made vulnerable as a result of the emergency”.
These divisions and distinctions between levels and types of vulnerability are not new. Our welfare system is based on demonstrating sufficient vulnerability to qualify for help. If you’re not vulnerable enough, you’re not eligible. Too vulnerable and your options are restricted because your needs are too high/complex.
Protect ‘the vulnerable’
Alongside the dehumanising and othering consequences, as soon as the vulnerable label is applied, any sense of power, agency or choice is removed from you, and you’re screened, sorted, prioritised and processed down a predetermined pathway. ‘Doing to’ is not just legitimised but celebrated. Just look at the narratives around the ‘brave heroes’ who ‘look after’, ‘protect’, ‘care for’ and indeed ‘save’ ‘the vulnerable’.
The rapid growth of ‘mutual aid’ groups during the pandemic has been recognised as one positive outcome of this horrific time. There are numerous examples of connections and relationships flourishing as WhatsApp groups and Facebook pages and notes through doors have united streets and led to conversations and company, shopping trips and prescription collections, seeds and garden plants shared, meals exchanged and lives no doubt enhanced and indeed saved. The growth of neighbours looking out for each other and caring about one another certainly gives us hope for a better future. There’s much to celebrate, and to sustain – but with a note of caution too. For it seems that the concept of ‘mutual’ – as in reciprocal/shared/equal – has sometimes got lost along the way. While the Covid-19 Mutual Aid UK network’s website emphasises that mutual aid “isn’t about “saving” anyone; it’s about people coming together, in a spirit of solidarity, to support and look out for one another”, its strapline is “Local organising to support the most vulnerable in our communities” [10]. And indeed, the media have been keen to celebrate the mutual aid groups springing up to “help the vulnerable”.
What term should we use instead?
Whether we’re ignoring, othering, ranking or fixing – what we’re not doing is helping. As with all labels, attaching them dehumanises, stereotypes and blames ‘broken’ people rather than focusing attention on broken systems.
What we don’t need to do is replace one label with another. And while replacing ‘vulnerable’ with ‘valuable’ is obviously a positive and powerful substitution [11], ultimately it is just another label. Another judgement that becomes much less appealing once it’s subject to the same ‘the valuable’, ‘most valuable’, ‘more valuable’, ‘not valuable enough’ interpretation.
What we do need to do is recognise that vulnerability is created by politics and policies and prejudice and power dynamics. Back to Matt Hancock’s “we recognise that people in social care were uniquely vulnerable”. If we take the “in social care” to mean in care homes (the ‘social care as a destination’ framing) what exactly is it that makes people living in care homes “uniquely vulnerable”? Age? Multiple comorbidities? Ability to understand and follow social distancing rules – either due to mental capacity or communal living arrangements? Maybe. But back in April Dr Hans Kluge, Regional Director of WHO Europe, suggested (in an address about COVID-19 in long-term care facilities) that “Even among very old people who are frail and live with multiple chronic conditions – many have a good chance of recovery if they are well-cared for.” [12]
I have no doubt that most people living in care homes have been exceptionally well cared for – and cared about – by dedicated and compassionate (and low paid and undervalued) care workers. What has made people living in care homes “uniquely vulnerable” from COVID-19 are the delays in implementing lockdown, the policies and pressures around hospital discharge, the lack of personal protective equipment (PPE), the failures around testing and the inadequate guidance around infection prevention and control – not to mention the wider, longer-term legacy of decades of underinvestment, bureaucratic systems and institutional ‘care’ becoming our default service solution. All of which is evidence that ultimately people “in social care” are not well-cared for (or about) at all.
So, have labels cost lives?
It could be argued that labels have saved lives during this time – galvanising people to work together – and indeed to stay apart – to ‘protect the vulnerable’. But use of the term vulnerable has undoubtedly also negatively influenced policy, attitudes, and behaviour. It has stifled debate and deflected attention from the systems, structures and prejudices that cause and perpetuate vulnerability. It’s justified paternalistic ‘fixing’ and denied people a voice and a choice. And it’s accentuated the ‘them and us’ divide.
I can’t help thinking that if, instead of ‘protect the NHS’ and ‘protect the vulnerable’ (them), the core message had been to ‘protect each other’ (us), we’d have experienced fewer divisions and maybe – just maybe – saved lives.
References
[1] New words list April 2020, Oxford English Dictionary
[2] COVID-19: review of disparities in risks and outcomes, Public Health England, 2 June 2020
[3] Who’s at higher risk from coronavirus, NHS, July 2020
[4] Protecting vulnerable people during the COVID-19 outbreak, Local Government Association, 3 April 2020
[5] ‘Widespread confusion and anxiety’ over lockdown easing, says Sheffield watchdog, Lucy Ashton, The Star, 10 June 2020
[6] Health and Social Care Secretary’s statement on coronavirus (COVID-19): 8 June 2020, Department of Health and Social Care, 9 June 2020
[7] Coronavirus: Hard to prevent care home deaths, says Chris Whitty, BBC News, 22 April 2020
[8] Coronavirus (COVID-19): Shielded patients list, NHS Digital, 17 July 2020
[9] Get coronavirus support as a clinically extremely vulnerable person, GOV.UK
[10] COVID-19 mutual aid
[11] Met with a yr10 boy last week… Viki, Twitter, 19 April 2020
[12] Statement – Invest in the overlooked and unsung: build sustainable people-centred long-term care in the wake of COVID-19, Dr Hans Henri P. Kluge, World Health Organisation Europe, 23 April 2020

Leave a comment